
If you’ve landed here, chances are you’re tired. Maybe confused. Possibly a little irritated that something so tiny could cause so much fuss.
A tongue tie, really?
And yet, here you are. Because feeding hurts. Or your baby clicks when nursing. Or weight gain is slow. Or someone casually said, “Have you checked for a tongue tie?” and now you can’t unhear it.
Here’s the thing: tongue ties aren’t new. But the conversation around them has changed. More parents are asking questions. More professionals are paying attention. And yes, there’s disagreement, sometimes loud disagreement, about what matters and what doesn’t.
Let me explain it calmly, carefully, and without scare tactics.
First Things First: What Is a Tongue Tie?
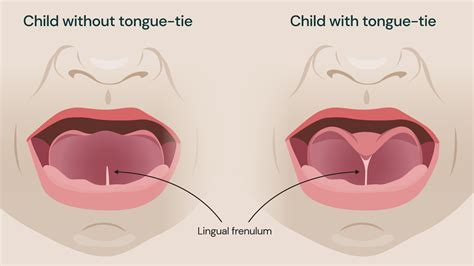
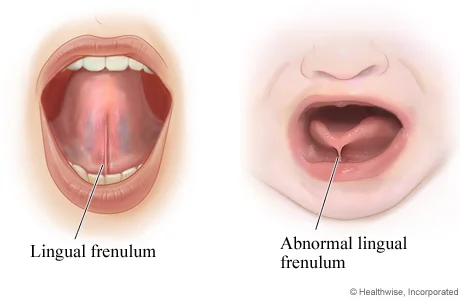
A tongue tie, medically called ankyloglossia, happens when the thin band of tissue under the tongue (the frenulum) is shorter, thicker, or tighter than usual. That band connects the tongue to the floor of the mouth.
When it’s too restrictive, the tongue can’t move the way it needs to.
That’s the technical version. The real-life version? The tongue acts like it’s tethered.
Now, a quick but important note: everyone has a frenulum. The presence of one doesn’t mean there’s a problem. It’s about function, not just appearance.
That distinction matters more than you might expect.
“But My Baby Sticks Their Tongue Out Fine” And Other Common Assumptions
This is where things get tricky.
A baby can sometimes stick out their tongue and still have a tongue tie that affects feeding. Why? Because feeding requires coordinated movement, lifting, cupping, extending, and retracting the tongue rhythmically.
It’s like saying someone can move their arm, so their shoulder must be fine. Movement alone doesn’t tell the full story.
Honestly, this is where a lot of parents feel dismissed. And understandably so.
The Different Types of Tongue Ties (Yes, There’s More Than One)
Not all tongue ties look the same. Some are obvious at first glance. Others hide in plain sight.
Anterior Tongue Ties
These are the classic ones. The frenulum attaches near the tip of the tongue and is easy to spot. The tongue may look heart-shaped when lifted.
Posterior Tongue Ties
These are deeper, subtler, and more controversial. The restriction is further back, often under a layer of tissue. You won’t always see it—you feel it in function.
Some professionals recognise posterior ties readily. Others remain sceptical. Both camps have reasons. But parents live with the outcomes, so the debate feels personal.
Submucosal Ties
Even trickier. Covered by a mucous membrane. Functionally restrictive, visually sneaky.
You know what? If this already sounds confusing, that’s normal. Most parents don’t learn this in one sitting. It unfolds over weeks, sometimes months.
How Tongue Ties Show Up in Babies (The Subtle Signs Matter)
Some signs wave red flags. Others whisper.
Feeding-Related Clues
- Painful latch (often described as pinching or burning)
- Clicking sounds during feeding
- Frequent breaks at the breast or bottle
- Long feeds, yet the baby still seems hungry
- Poor weight gain—or oddly, rapid gain with constant feeding
Baby Behaviour You Might Notice
- Gassy, uncomfortable feeds
- Arching or fussiness at the breast
- Falling asleep quickly while feeding
- Milk leaking from the corners of the mouth
And here’s a curveball: some babies compensate. They muscle through. Feeding “works,” but it’s inefficient and exhausting for everyone involved.
Breastfeeding, Bottle-Feeding, and Tongue Ties: No One-Size Story
Breastfeeding gets most of the attention, and for good reason. It’s mechanically complex. The tongue plays a starring role.
But bottle-fed babies can struggle too. Reflux-like symptoms, choking, and excessive air intake are not exclusive to nursing.
Parents sometimes feel brushed off if they’re not breastfeeding. That’s unfortunate. Feeding is feeding. Strain is strain.
And yes, tongue ties can affect solids later, gagging, texture refusal, and slow progression. It’s all connected.
Let’s Pause for the Emotional Side (Because It’s Real)
This part doesn’t get enough space.
Parents, especially new mothers, often blame themselves. “If I were better at this…” “If my body worked right…”
That guilt is heavy. And unnecessary.
Tongue ties aren’t caused by parenting choices. They’re anatomical variations. Full stop.
You’re not failing. You’re noticing.
Diagnosis: Who Spots a Tongue Tie?
Sometimes it’s:
- A lactation consultant
- A pediatric dentist
- A speech-language therapist
- A paediatrician (less often, but it happens)
The keyword here is trained. Not everyone assesses tongue function deeply. That’s not incompetence, it’s scope and experience.
A thorough evaluation looks at:
- Tongue lift
- Lateral movement
- Extension
- Suck pattern
- Feeding observation
A quick peek isn’t enough. If someone diagnoses or dismisses a tongue tie in under 30 seconds without watching a feed, it’s okay to ask for more.
Treatment Options: From Watchful Waiting to Procedures
This is where opinions diverge.
When No Treatment Is Needed
Some tongue ties don’t cause functional issues. If feeding is comfortable, growth is steady, and development is on track, doing nothing can be perfectly reasonable.
Yes, really.
Supportive Therapy
- Lactation support
- Oral motor exercises
- Positioning adjustments
For mild cases, this can be enough.
Frenotomy or Frenectomy
A quick procedure that releases the frenulum. It can be done with scissors or a laser, depending onthe provider’s preference.
It’s fast. Often seconds long. Babies usually feed immediately afterwards.
But, and this matters, it’s not a magic fix. Aftercare and follow-up are crucial.
Recovery: What Actually Happens After Release
Some babies feed better right away. Others take days or weeks.
There may be:
- Temporary fussiness
- Increased need for comfort
- Exercises to prevent reattachment
This surprises parents. They expect instant relief. Sometimes that happens. Sometimes progress is gradual, layered, and a bit messy.
That doesn’t mean it didn’t work.
Beyond Feeding: Speech, Sleep, Teeth, and Posture
Here’s where the conversation expands.
Tongue movement influences:
- Speech clarity
- Jaw development
- Palate shape
- Breathing patterns
- Sleep quality
Not every tongue tie causes these issues. But when patterns stack—mouth breathing, snoring, delayed speech, it’s worth looking deeper.
Speech therapists often see older kids whose feeding issues were subtle but whose speech challenges are more obvious.
And adults? Many discover tongue ties during orthodontic work or sleep evaluations. Yes, really.
The Big Question: Is Tongue Tie Overdiagnosed?
Sometimes. And sometimes underdiagnosed.
Both can be true.
Awareness brings attention. Attention brings questions. Questions bring differing thresholds for action.
The goal isn’t to label every frenulum a problem. It’s to respect function, symptoms, and family experience.
You’re allowed to weigh options. You’re allowed to pause. You’re allowed to seek another opinion.
Questions Parents Ask (Usually Whispered)
“Did I miss this earlier?”
Probably not. Many signs only appear as demands increase.
“Will my baby grow out of it?”
Sometimes compensation happens. True resolution varies.
“Is it my fault?”
No. No. And no again.
“Why didn’t anyone tell me?”
Because medicine evolves. And so does awareness.
Trust Your Instincts. But Ground Them in Support
Here’s the gentle truth: parents are often the first to sense something’s off. That instinct deserves respect. Pair it with skilled evaluation, and you’re in solid territory.
Tongue ties aren’t a trend. They’re not a diagnosis to chase or fear. They’re one piece of a bigger feeding and development puzzle.
And you don’t have to solve it alone.
If this article gave you clarity, or at least calmer questions, that’s a good place to be. Take a breath. You’re doing better than you think.
